what causes the femural nrve to become irritaded when sitting
Original Editors - Marlies Verbruggen
Pinnacle Contributors - Marlies Verbruggen, Vidya Acharya, Admin, Kudzanayi Ronald Muzenda, Kim Jackson, Ajay Upadhyay, Rachael Lowe, Maëlle Cormond, WikiSysop, Daphne Jackson, Carolie Siffain, Claire Knott, Simisola Ajeyalemi, Wanda van Niekerk and Kai A. Sigel
Definition/Description [edit | edit source]
Piriformis syndrome (PS) is a painful musculoskeletal condition, characterized by a combination of symptoms including buttock or hip pain.[1] [two] [3] In several manufactures, piriformis syndrome is defined as a peripheral neuritis of the branches of the sciatic nervus caused by an aberrant condition of the piriformis muscle (PM), such as an injured or irritated muscle.[4] [3] Synonyms that are used frequently for PS are the deep gluteal syndrome, extra-spinal sciatica, wallet neuritis, etc[5]. At that place are more than women diagnosed with Piriformis syndrome than men, with a female–to–male ratio of 6:1. This ratio tin can be explained past the wider quadriceps femoris musculus angle in the os coxae of women.[half dozen] [vii] [3]
Clinically Relevant Beefcake [edit | edit source]
The piriformis muscle (PM) originates from the pelvic surface of the sacral segments S2-S4 in the regions between and lateral to the inductive sacral foramina, the sacroiliac joint (superior margin of the greater sciatic notch), the anterior sacroiliac ligament and occasionally the anterior surface of the sacro-tuberous ligament. It passes through the greater sciatic notch to insert onto the greater trochanter of the femur.
The PM is functionally involved with external rotation, abduction and fractional extension of the hip.[viii] [9]
The sciatic nerve generally exits the pelvis below the belly of the muscle, notwithstanding many congenital variations may exist.[nine]
The relationships betwixt the PM and sciatic nervus have been classified by Beaton and Anson using a six category classification system[10]. An anomalous relationship would exist labelled betwixt type ''B'' through type ''F'' since type ''A'' is considered to accept a normal relationship between the PM and the sciatic nerve.[xi]
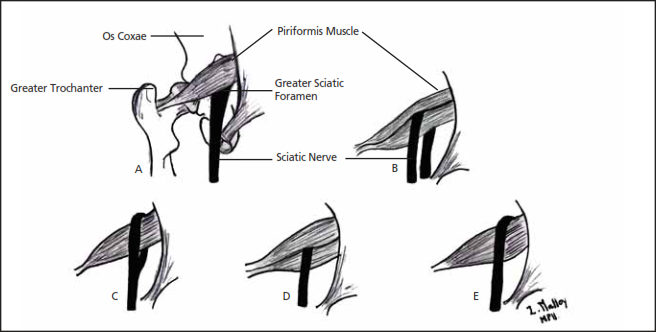
Relationship of Sciatic nerve to Piriformis
Variations in the relationship of the sciatic nerve to the piriformis musculus shown on the diagram higher up:
- The sciatic nerve exiting the greater sciatic foramen along the junior surface of the piriformis musculus; the sciatic nervus splitting as information technology passes through the piriformis muscle with the tibial branch passing;
- Inferiorly or
- Superiorly;
- The entire sciatic nerve passing through the muscle abdomen;
- The sciatic nerve exiting the greater sciatic foramen along the superior surface of the piriformis muscle. The nerve may also divide proximally, where the nerve or a division of the nervus may pass through the belly of the muscle, through its tendons or between the part of a congenitally bifid muscle.[3]
Epidemiology /Aetiology [edit | edit source]
According to Boyajian- O' Neill L.A. et al., at that place are two types of piriformis syndrome- primary and secondary[3].
Primary Piriformis Syndrome [edit | edit source]
Chief piriformis syndrome has an anatomical cause, with variations such equally a split up piriformis musculus, separate sciatic nerve, or an anomalous sciatic nerve path. Among patients with piriformis syndrome, fewer than 15% of cases have primary causes.[3] At present, in that location are no accepted values for the prevalence of the anomaly and niggling show to support whether or not the bibelot of the sciatic nervus causes piriformis syndrome or other types of sciatica.[11] These findings suggest that piriformis and sciatic anomalies may not exist as important to the pathophysiology of piriformis syndrome as previously idea.[11]
Secondary Piriformis Syndrome [edit | edit source]
Secondary piriformis syndrome occurs as a result of a precipitating cause, including macrotrauma, microtrauma, ischemic mass event, and local ischemia.
- Piriformis syndrome is nearly frequently (50% of the cases) caused by macrotrauma to the buttocks, leading to inflammation of soft tissue, musculus spasms, or both, with resulting nerve compression.
- Muscle spasms of the PM are well-nigh often caused by direct trauma, post-surgical injury, lumbar and sacroiliac joint pathologies or overuse.[4] [6] [7] [ii] [3]
- PS may likewise exist acquired by shortening of the muscles due to the contradistinct biomechanics of the lower limb, depression dorsum and pelvic regions [8]. This tin consequence in compression or irritation of the sciatic nervus. [4] [vii] [9] When there is a dysfunction of the piriformis musculus, it can cause various signs and symptoms such as pain in the sciatic nerve distribution, including the gluteal expanse, posterior thigh, posterior leg and lateral aspect of the foot.[6]
- Microtrauma may result from overuse of the piriformis musculus, such equally in long-distance walking or running or past direct compression. An example of this kind of straight compression is known as "wallet neuritis", which is a repetitive trauma caused by sitting on difficult surfaces.[3]
Aetiology of the piriformis syndrome [12]
| Gluteal trauma in the sacroiliac or gluteal areas | predisposing anatomic variants |
| Myofascial trigger points | Hypertrophy and spasm of the piriformis muscle |
| Secondary to laminectomy | Abcess, hematoma, myositis |
| Bursitis of the piriformis muscle | Neoplasms in the expanse of the infrapiriform foramen |
| Colorectal carcinoma | Neurinoma of the sciatic nerve |
| Episacroiliac lipoma | Intragluteal injection |
| Femoral nailing | Myositis ossificans of the piriformis musculus |
| Klippel-Trénaunay syndrome |
Other causative factors are anatomic variations of the divisions of the sciatic nerve, anatomic variations or hypertrophy of piriformis muscle, repetitive trauma, sacro-iliac arthritis and total hip replacement.[6] [vii] [thirteen] [2] A Morton's Toe tin too predispose the patient to develop piriformis syndrome. A fraction of the population is at high hazard, particularly skiers, truck drivers, tennis players and long-distance bikers.[6]
Tonley JC[iv] had another view almost the causes of PS. He mentioned: "The piriformis musculus may be operation in an elongated position or subjected to high eccentric loads during functional activities secondary to weak agonist muscles. For instance, if the hip excessively adducts and internally rotates during weight-bearing tasks, due to the weakness of the gluteal maximus and/or the gluteus medius, a greater eccentric load may be shifted to the piriformis musculus. Perpetual loading of the piriformis muscle through overlengthening and eccentric need may result in sciatic nervus compression or irritation".[iv]
Characteristics/Clinical Presentation [edit | edit source]
Patients with piriformis syndrome have many symptoms that typically consist of persistent and radiating low dorsum hurting, (chronic) buttock hurting, numbness, paraesthesia, difficulty with walking and other functional activities such as pain with sitting, squatting, standing, with bowel movements and dyspareunia in women.[4] [6] [1] [13] [3] [14] [15]. Other characteristics include the post-obit:
- They can also take pressure level pain in the buttock on the aforementioned side as the piriformis lesion and betoken tenderness over the sciatic notch in almost all instances. The buttock pain can radiate into the hip, the posterior aspect of the thigh and the proximal portion of the lower leg.[4] [fourteen]
- Swelling in the legs and disturbances of sexual functions have also been observed in patients with PS.[14]
- There may be an aggravation of hurting with activeness, prolonged sitting or walking, squatting, hip adduction and internal rotation and manoeuvers that increment the tension of the piriformis muscle.[iv] [6] [1] [13]
- Depending on the patient, the pain tin lessen when lying down, angle the knee or when walking. Still, some patients cannot tolerate the pain in any position and can just detect relief when they're walking.[15] [14]
- Piriformis syndrome is non characterized by neurological deficits typical of a radicular syndrome, such as declined deep tendon reflexes and myotomal weakness.
- The patient may present with a limp when walking or with their leg in a shortened and externally rotated position while supine[1] [14]. This external rotation while supine tin can be a positive piriformis sign, likewise called a splayfoot. Information technology tin can exist the result of a contracted piriformis muscle.[seven] [3]
Differential Diagnosis [edit | edit source]
Piriformis syndrome can "masquerade" as other common somatic dysfunctions such equally:
- Thrombosis of the iliac vein[ii]
- Trochanteric Bursitis[3]
- Painful vascular pinch syndrome of the sciatic nerve, caused by gluteal varicosities
- Herniated intervertebral disc[3]
- Post-laminectomy syndrome or coccygodynia[4]
- Posterior facet syndrome at L4-5 or L5-S1[six]
- Unrecognized pelvic fractures[7]
- Lumbar osteochondrosis
- Undiagnosed renal stones
- Lumbosacral radiculopathies
- Osteoarthritis (lumbosacral spine)
- Sacroiliac joint syndrome
- Degenerative disc affliction
- Compression fractures
- Intra-articular pathology in the hip joint: labral tears [11], femuro-acetabular impingement (FAI)[15]
- Lumbar spinal stenosis
- Tumours, cysts
- Gynaecological weather condition
- Diseases such as appendicitis, pyelitis, hypernephroma, uterine disorders, prostate disorders and malignancies in pelvic viscera.
- Dysfunction, lesion and inflammation of sacroiliac joint[i]
- Pseudoaneurysm in the inferior gluteal artery post-obit gynaecological surgery
- Sacroiliitis[14] [xvi] [12] [4]
- Psychogenic disorders: concrete fatigue, depression, frustration
Investigations [edit | edit source]
Piriformis syndrome continues to exist a controversial diagnosis for sciatic hurting.
Radiographic studies have limited application to the diagnosis of piriformis syndrome. Although standard anteroposterior radiographs of the pelvis and hips, lateral views of the hips and either CT or MRI of the lumbar spine are recommended to dominion out the possibility that the symptoms experienced by the patients originate from the spine or the hip joint.[12]
Electromyography (EMG) may be likewise benign in differentiating piriformis syndrome from other possible disorders, such as intervertebral disc herniation. Interspinal nervus impingement will cause EMG abnormalities of muscles proximal to the piriformis muscle. In patients with piriformis syndrome, however, EMG results will be normal for muscles proximal to the piriformis musculus and aberrant for muscles distal to it. Electromyography examinations that incorporate active manoeuvers, such equally the FAIR test, may take a greater specificity and sensitivity than other bachelor tests for the diagnosis of piriformis syndrome[3]
Electrophysiological testing and nervus blocks play important roles when the diagnosis is uncertain. Injection of local anaesthetics, steroids, and botulinum toxin into the piriformis musculus tin serve both diagnostic and therapeutic purposes[12].
Outcome Measures [edit | edit source]
Roland-Morris Disability Questionnaire
Examination [edit | edit source]
A complete neurological history and physical assessment of the patient is essential for an accurate diagnosis. The physical assessment should include the following points:
- an osteopathic structural examination with special attending to the lumbar spine, pelvis and sacrum, as well as any leg length discrepancies
- diagnostic tests
- deep-tendon reflex testing, strength and sensory testing
Diagnostic tests [edit | edit source]
Observation [edit | edit source]
Patients with piriformis syndrome may also present with gluteal atrophy, besides every bit shortening of the limb on the afflicted side.In chronic cases, muscle hypotrophy is present in the afflicted extremity.
Palpation [edit | edit source]
The patient reports sensitivity during palpation at the greater sciatic notch, in the region of sacroiliac joint or over the piriformis musculus belly. Information technology is possible to observe the spasm of the PM by careful, deep palpation.[7] [i] [nine]
With deep digital palpation in the gluteal and retro-trochanteric area, there may be tenderness and pain with an exacerbation of tightness and leg numbness.[16]
Pace sign [edit | edit source]
Pace's sign consists of hurting and weakness past resisted abduction and external rotation of the hip in a sitting position. A positive examination occurs in 46.5% of the patients with piriformis syndrome.[half-dozen] [one] [3] [12]
Lasèque sign / Straight Leg Raise Test [12] [edit | edit source]
The patient reports buttock and leg pain during passive a directly leg enhance performed by the examiner.[16]
Freiberg Sign [edit | edit source]
Involves pain and weakness on passive forced internal rotation of the hip in the supine position. The pain is thought to be a result of passive stretching of the piriformis muscle and pressure level placed on the sciatic nerve at the sacrospinous ligament. Positive in 56,2% of the patients.[12]
Off-white [edit | edit source]
Painful flexion-adduction-internal rotation [sixteen]
[17]
Beatty's Manoeuver [edit | edit source]
An active examination that involves elevation of the flexed leg on the painful side, while the patient is lying on the asymptomatic side. The abduction causes deep buttock pain in patients with PS, but dorsum and leg pain in patients with lumbar disc affliction.[12]
The Hughes test [edit | edit source]
External isometric rotation of the afflicted lower extremity following maximal internal rotation may also exist positive in PS patients.[12]
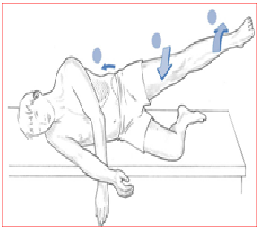
Hip Abduction Test [edit | edit source]
The patient lies on the side with lower leg flexed to provide support and the upper leg direct, in line with the body. The practitioner stands in forepart of the patient at the level of the anxiety and observes (no hands-on) as the patient is asked to abduct the leg slowly.
Normal – Hip abduction to 45°.
Abnormal – if hip flexion occurs (indicating TFL shortness) and/or leg externally rotates (indicating piriformis shortening) and/or 'hiking' of the hip occurs at the commencement of the move (indicating quadratus overactivity and therefore, by implication, shortness)
Trendelenburg Sign [edit | edit source]
Trendelenburg sign may as well be positive.[16]
Medical Direction [edit | edit source]
Conservative handling for piriformis syndrome includes pharmacological agents [non-steroidal anti-inflammatory agents (NSAIDs), muscle relaxants and neuropathic pain medication], physical therapy, lifestyle modifications and psychotherapy.[12]
Injections of local anaesthetics, steroids, and botulinum toxin into the PM musculus can serve both diagnostic and therapeutic purposes. The practitioner should be familiar with variations in the anatomy and the limitations of landmark-based techniques. An ultrasound-guided injection technique has recently been utilized. This technique has been shown to have both diagnostic and therapeutic value in the treatment of PS.[12]
Piriformis syndrome oftentimes becomes chronic and pharmacological treatment is recommended for a short time period.[16]
Surgical Management [edit | edit source]
Surgical interventions should exist considered only when nonsurgical handling has failed and the symptoms are condign intractable and disabling. Classic indications for surgical treatment include abscess, neoplasms, hematoma, and painful vascular pinch of the sciatic nerve caused by gluteal varicosities.[12]
Surgical release with tenotomy of the piriformis tendon to save the nerve from the pressure of the tense muscle has resulted in immediate pain relief, as reported past several authors.
Sometimes, the obturator internus muscle should be considered as a possible cause of sciatic pain. Nevertheless, the diagnosis of the obturator internus syndrome can only exist made past ruling out other possible causes of sciatic hurting, which is similar to the manner in which piriformis syndrome is diagnosed.[sixteen] Surgical release of the internal obturator muscle can result in both a short- and long-term reduction in hurting in patients with retro-trochanteric hurting syndrome and should be considered if conservative treatment fails.
The postoperative management consists of partial weight-bearing using crutches for 2 weeks and unrestricted range of motion exercises. The above surgical approach has shown promising short-term results[sixteen]
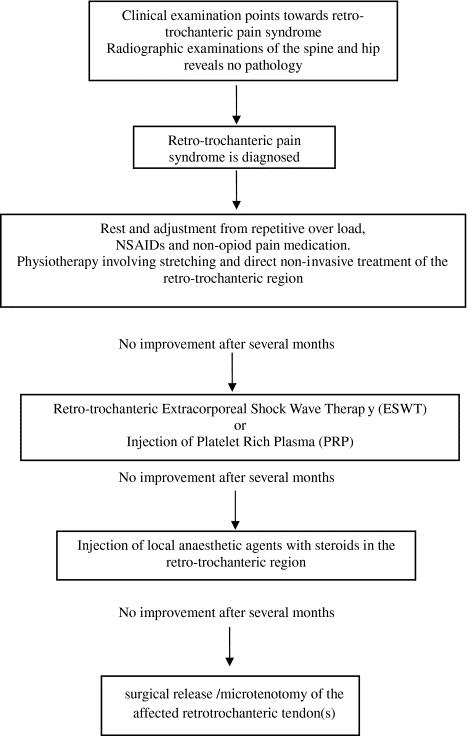
The treatment algorithm for retro-trochanteric pain syndrome:
Physical Therapy Direction [edit | edit source]
Although there is a paucity of recently published controlled trials in which critically examine the effectiveness of the noninvasive management modalities[12], a number of methods exist for the treatment of 'Piriformis Syndrome'.
The non-invasive treatments include physical therapy, (osteopathic) manipulative handling [iii] and lifestyle modification[12]. The use of Ozone Therapy can exist considered in the management of PS, due to the absence of side furnishings, the practicality of use and the extent of clinical improvement[eighteen].
According to Tonley et al., the most commonly reported physical therapy interventions include ultrasound, soft tissue mobilization, piriformis stretching, hot packs or cold spray and diverse lumbar spine treatments. In addition, Tonley et al. describe an alternative treatment approach for piriformis syndrome. The intervention focused on functional exercises Therapy Exercises for the Hipaimed at strengthening the hip extensors, abductors and external rotators, too as correction of faulty movement patterns. Despite positive outcomes full resolution of low back pain, cessation of buttock and thigh hurting in the single instance report intendance must be taken in establishing cause and effect based on a single patient. Further investigation is needed[iv]
To accomplish a 60 – 70% improvement, the patient usually follows two – iii treatments weekly for 2-iii months[19].
- First of all, the patient must be placed in the contralateral decubitus and Off-white position (Flexed Adducted Internally Rotated). Commencement with an ultrasound treatment: 2.0-ii.5 W/cm2, for 10-14 minutes. Apply the ultrasound gel in broad strokes longitudinally along the piriformis muscle from the conjoint tendon to the lateral border of the greater sciatic foramen.[4] [6] [2] [3]
- Earlier stretching the piriformis musculus, treat the same location with hot packs or cold spray for 10 minutes. The use of hot and common cold before stretching is very useful to decrease pain. [4] [vi] [iii]
- Later on that, brainstorm with stretching of the piriformis which can be executed in a variety of ways. Stretch the piriformis muscle by applying manual pressure to the muscle's inferior border. It is of import not to press downward, rather directing pressure level tangentially, toward the ipsilateral shoulder. When pressing down, the sciatic nerve will compress against the tendinous edge of the gemellus superior. However, when applying tangential pressure, the muscle's grip volition weaken on the nervus and relieve the hurting of the syndrome.[4] [three] (18, Fischman et al. (2002), level of evidence A2), Some other way to stretch this muscle is in the FAIR position. The patient lies in a supine position with the hip flexed, adducted and internally rotated. And so the patient brings his foot of the involved side beyond and over the articulatio genus of the uninvolved leg. We can enhance the stretch, past letting the physical therapist perform a muscle–energy technique. This technique involves the patient abducting his limb against calorie-free resistance, which is provided by the therapist for v-7 seconds, with 5-7 repetitions.[vi] [seven] [19]
[twenty]
- After stretching, go along with myofascial release at the lumbosacral paraspinal muscles and McKenzie exercises. When the patient lies in the Off-white position, the lumbosacral corset can be used.[3] [19]
- PS is caused when the tight piriformis is forced to do the work of other big muscles (like the gluteus maximus, the gluteus medius), An alternative treatment[4] arroyo for piriformis syndrome using a hip muscle strengthening programme especially of the weak gluteal musculature with move re-didactics can help in pain relief.
[21]
The therapist can also give several tips to avoid an aggravation of the symptoms. This includes:
- Avoid sitting for a long period; stand and walk every 20 minutes,
- Make frequent stops when driving to stand up and stretch.
- Prevent trauma to the gluteal region and avoid farther offending activities.
- Daily stretching is recommended to avoid the recurrence of the piriformis syndrome.[six] [vii] [3]
Home exercises: [edit | edit source]
The patient can too perform several exercises and treatments at domicile including:
- Rolling side to side with flexion and extension of the knees while lying on each side
- Rotate side to side while standing with the arms relaxed for i minute every few hours
- Accept a warm bath
- Prevarication flat on the dorsum and enhance the hips with your hands and pedal with the legs similar you are riding a bicycle.
- Knee bends, with equally many as 6 repetitions every few hours.[6]
Clinical Bottom Line [edit | edit source]
Piriformis syndrome (PS) is a painful musculoskeletal status and is most often caused past macrotrauma to the buttocks, leading to inflammation of soft tissue, muscle spasms, or both, with resulting nerve compression. Patients with piriformis syndrome have many symptoms that typically consist of persistent and radiating low back pain, (chronic) buttock hurting, numbness, paraesthesia, difficulty with walking and other functional activities. Piriformis syndrome continues to be a controversial diagnosis for sciatic pain. A complete neurological history and physical assessment of the patient is essential for an accurate diagnosis. Optimizing the therapeutic approach requires an interdisciplinary evaluation of treatment.
References [edit | edit source]
- ↑ one.0 1.1 ane.two 1.iii 1.4 i.5 1.6 Kirschner JS, Foye PM, Cole JL. Piriformis syndrome, diagnosis and handling. Muscle Nerve Jul 2009;40(one):10-18
- ↑ 2.0 2.one ii.2 2.3 2.four Balk F, Bottrell O, et al. Non–surgical direction of piriformis syndrome: A systematic review. Phys Ther Rev 2007;12:66-72. ( A1)
- ↑ 3.00 iii.01 3.02 3.03 iii.04 3.05 3.06 three.07 three.08 iii.09 3.10 three.eleven 3.12 3.13 iii.14 3.15 3.16 three.17 3.18 3.nineteen Boyajian-O'Neill LA, McClain RL, Coleman MK, Thomas PP. Diagnosis and management of piriformis syndrome:an osteopathic arroyo. The Periodical of the American Osteopathic Association. 2008 November one;108(eleven):657-64
- ↑ 4.00 4.01 4.02 4.03 4.04 four.05 4.06 4.07 four.08 four.09 4.x 4.11 4.12 4.13 4.14 Tonley JC, Yun SM, et al. Treatment of an individual with piriformis syndrome focusing on hip muscle strengthening and movement reeducation: a case written report. J Orthop Sports Phys Ther 2010;40(2):103-111.
- ↑ Siddiq MA. Piriformis Syndrome and Wallet Neuritis: Are They the Same?. Cureus. 2018 May;x(5).
- ↑ vi.00 6.01 6.02 vi.03 6.04 vi.05 half dozen.06 6.07 6.08 half dozen.09 half dozen.ten 6.eleven half dozen.12 6.xiii Shah S, Wang TW. Piriformis syndrome. eMedicine specialities: Sports medicine: hip 2009 fckLR http://emedicine.medscape.com/article/87545-overview
- ↑ 7.0 7.1 7.two seven.three 7.four seven.v vii.vi 7.7 7.8 Klein MJ. Piriformis syndrome. eMedicine Specialities: Physical Medicine and Rehabilitation: Lower limb Musculoskeletal conditions 2010 fckLR http://emedicine.medscape.com/article/308798-overview
- ↑ viii.0 eight.1 Chapman C, Bakkum BW. Chiropractic management of a U.s.a. Army veteran with depression back hurting and piriformis syndrome complicated by an anatomical anomaly of the piriformis muscle: a case written report. Journal of chiropractic medicine. 2012 Mar i;11(1):24-9.
- ↑ nine.0 9.ane 9.2 nine.3 Hopayian One thousand, Song F, Riera R, Sambandan S. The clinical features of the piriformis syndrome: a systematic review. European Spine Periodical. 2010 December 1;19(12):2095-109.
- ↑ Beaton LE, Anson BJ. The relation of the sciatic nervus and of its subdivisions to the piriformis musculus. The Anatomical Record. 1937 Dec;70(ane):1-5.
- ↑ 11.0 11.1 eleven.2 eleven.3 Smoll NR. Variations of the piriformis and sciatic nerve with clinical consequence: a review. Clinical Anatomy: The Official Journal of the American Association of Clinical Anatomists and the British Association of Clinical Anatomists. 2010 January;23(1):8-17.
- ↑ 12.00 12.01 12.02 12.03 12.04 12.05 12.06 12.07 12.08 12.09 12.x 12.11 12.12 12.13 Jankovic D, Peng P, van Zundert A. Brief review: piriformis syndrome: etiology, diagnosis, and management. Canadian Journal of Anesthesia/Periodical canadien d'anesthésie. 2013 Oct 1;60(ten):1003-12.
- ↑ xiii.0 13.one 13.2 Hopayian K. The clinical features of the piriformis syndrome. Surgical and radiologic anatomy. 2012 Sep ane:i-.
- ↑ xiv.0 14.ane xiv.ii 14.3 14.4 14.five Kunbong Choi, The etiology, diagnosis and handling of piriformis syndrome (2004)(5)
- ↑ 15.0 15.1 15.2 Conservative Management of Piriformis Syndrome Douglas Volume 27 * Number 2 * 1992 * Periodical of Athletic Training (2C)
- ↑ 16.0 16.one 16.ii sixteen.iii sixteen.four sixteen.5 16.six sixteen.7 Meknas K, Johansen O, Kartus J. Retro-trochanteric sciatica-like hurting: current concept. Knee Surgery, Sports Traumatology, Arthroscopy. 2011 Nov one;19(11):1971.
- ↑ TSPTblog Off-white Examination Available fromhttps://www.youtube.com/watch?time_continue=36&v=9Q9YdBke3Kc
- ↑ Valdenassi L, Bellardi D. Treatment of piriformis syndrome with oxygen-ozone therapy. Ozone Therapy. 2017 Dec 31;2(3).
- ↑ 19.0 nineteen.one 19.2 Fishman LM, Dombi GW, Michaelsen C, Ringel S, Rozbruch J, Rosner B, Weber C. Piriformis syndrome: diagnosis, treatment, and outcome—a 10-twelvemonth study. Archives of physical medicine and rehabilitation. 2002 Mar 1;83(iii):295-301.
- ↑ Hurting TherapySupine Piriformis Stretch Available from https://www.youtube.com/lookout?time_continue=61&v=eKp2f5-jRbI
- ↑ Lisa Gillispie Piriformis Stretch Bachelor at https://www.youtube.com/watch?v=mxZBSMdYGXc
Source: https://www.physio-pedia.com/Piriformis_Syndrome
0 Response to "what causes the femural nrve to become irritaded when sitting"
Post a Comment